What Families Get Wrong About Macular Degeneration
Common myths about macular degeneration, plus the facts on dry vs. wet AMD, early symptoms, the Amsler grid test, and treatment options.

For most families, the words "macular degeneration" land like a sentence. Someone pictures a parent going blind, losing the house, losing independence, all of it arriving at once. That fear is understandable, and it is almost entirely wrong. Age-related macular degeneration is the leading cause of central vision loss in older adults, and according to the Centers for Disease Control and Prevention, roughly 20 million Americans are living with some form of it. Yet only a small fraction have the advanced, vision-threatening stage, and even they rarely go completely blind.
The gap between what people fear and what actually happens is where families make their worst decisions, either panicking or, just as often, ignoring early signs because "nothing can be done anyway." Both come from myths. Here are the ones worth clearing up, and the facts that replace them.
Myth: A Diagnosis Means Going Blind
This is the fear that does the most damage, and it rests on a misunderstanding of what the macula does. The macula is a tiny patch at the center of the retina responsible for sharp, straight-ahead vision: reading, threading a needle, recognizing a face across the table. AMD attacks that center. It generally leaves the surrounding peripheral retina, the part you use to sense a room, notice movement, and find your way to the kitchen, largely intact.
So the realistic outcome of even serious AMD is not darkness. It is a blurred or missing spot in the middle of your gaze, with usable side vision around it. People learn to look slightly off-center to see, use magnifiers and brighter light, and keep doing far more than they expected. Legal blindness happens in advanced cases; total blindness is rare. That distinction changes everything about how a family plans, because the goal shifts from bracing for the worst to protecting the vision that will very likely remain.
Myth: It's Just Aging, So Nothing Can Be Done
The word "age-related" fools people into treating AMD as an inevitability to be endured, like gray hair. Age is indeed the biggest risk factor, and risk climbs steeply after 60. But several of the other major contributors are things you can act on. Smoking is the standout: it roughly doubles the risk and worsens the disease, which makes quitting the single most effective move at any age. High blood pressure, excess weight, a poor diet, and heavy sun exposure all add to the risk too.
Family history matters as well, so if AMD runs in the family, that is a reason to be more vigilant, not more fatalistic. A person who does not smoke, keeps their blood pressure controlled, eats leafy greens and fish, and gets a yearly dilated eye exam is genuinely stacking the odds in their favor. "Nothing can be done" is the belief that stops people from doing the several things that actually work.
Myth: Dry and Wet Are the Same Thing
Families often hear "macular degeneration" as one condition, but the two forms behave so differently that lumping them together leads to the wrong worries and the wrong plans. The distinction is the most useful thing you can learn about the disease.
| Dry AMD | Wet AMD |
|---|---|---|
| How common | About 80 percent of cases | Less common, but causes most severe vision loss |
| What happens | Macula slowly thins; deposits called drusen build up | Abnormal blood vessels grow and leak fluid or blood |
| Speed | Gradual, often over years | Fast, sometimes days to weeks |
| Main treatment | AREDS2 vitamins; newer injections for advanced cases | Anti-VEGF eye injections that can stabilize or improve vision |
The takeaway: dry AMD is the common, slow version, and wet AMD is the less common but more dangerous one that accounts for most severe loss. Dry AMD can also convert to wet, which is why anyone with dry AMD should know the emergency signs and keep monitoring. And counterintuitively, the scarier-sounding wet form is the more treatable, because the injections that address it are genuinely effective.
Myth: You'd Notice Right Away
People assume something as serious as macular degeneration would announce itself. It usually does not. AMD is painless, and in its early stages it produces no obvious symptoms at all. When changes do begin, the brain and the stronger eye quietly compensate, so a person can lose real ground in one eye without realizing it. That is exactly why AMD is so often caught late, at a routine exam or only after vision has clearly slipped.
When symptoms do appear, they show up in central vision. According to the National Eye Institute, the early warning signs include straight lines that look wavy or crooked, a blurry or empty spot in the middle of your vision, colors that seem faded, and a growing need for bright light to read. The two habits that catch this early are simple: get a dilated eye exam every year, and check each eye on its own, because covering the stronger eye is often the only way to notice a problem in the weaker one.
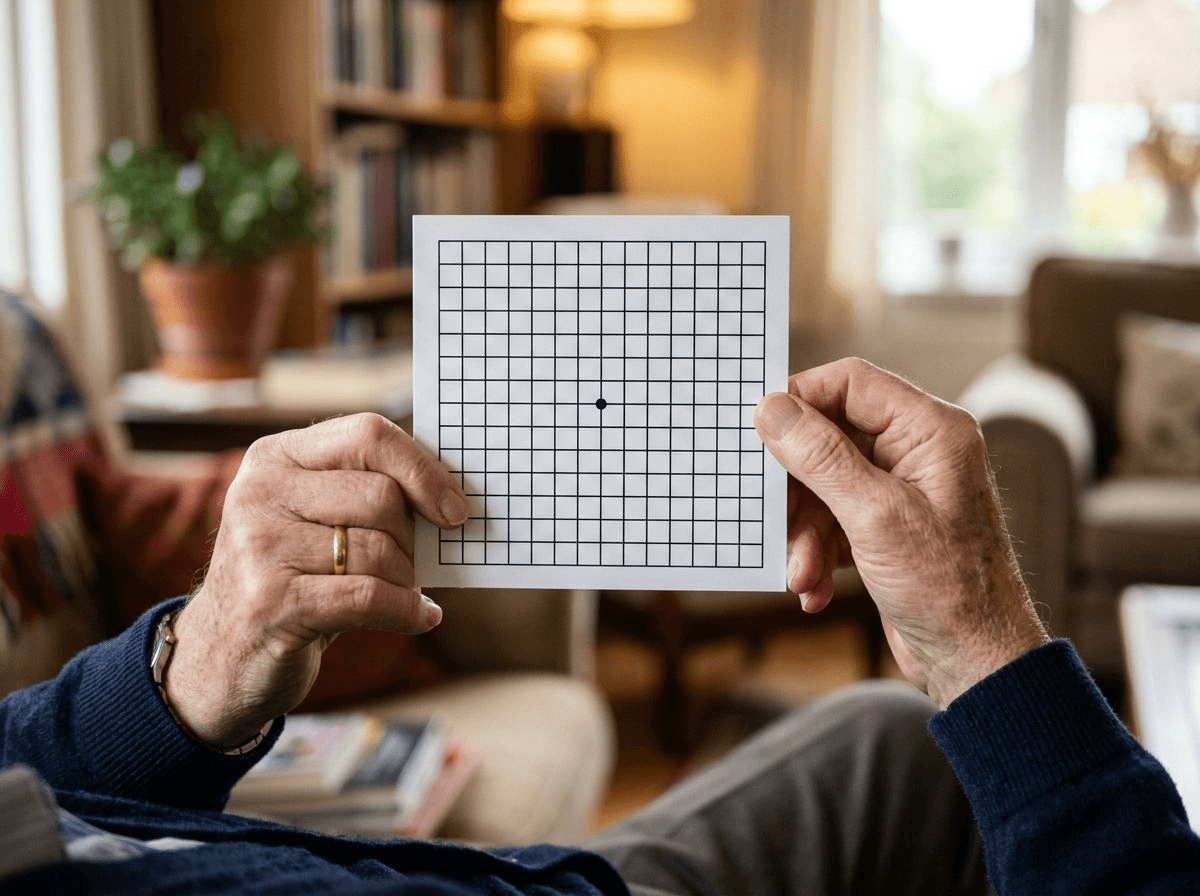
This is where the Amsler grid earns its keep. It is a simple square grid with a dot in the center, and it costs nothing. You hold it at reading distance in good light, wearing your usual reading glasses, cover one eye, and stare at the center dot. If any of the lines look wavy, blurry, faded, or missing, that is a reason to call an eye doctor promptly, especially if it is new, since sudden distortion can signal wet AMD that needs fast treatment. The American Academy of Ophthalmology recommends people at risk use one regularly at home. Taping it to the refrigerator and checking each eye a few times a week turns a slow, silent disease into something you can actually catch in time.
Myth: There's No Treatment
A generation ago this was closer to true, and the belief has stuck around long after the science moved on. Today the picture is very different depending on the form. For wet AMD, anti-VEGF injections, given directly into the eye on a schedule, block the leaky blood vessels driving the damage. They can stop the disease from worsening and, in many cases, recover some of the vision already lost. It sounds daunting, but the eye is numbed, and for people with wet AMD these injections are often the difference between keeping and losing central vision.
For dry AMD, the AREDS2 vitamin formula can slow the move from intermediate to advanced disease. And the advanced form of dry AMD, once untreatable, now has options: in 2023 the FDA approved the first injectable therapies for it, which slow the progression of the damage. These newer drugs slow decline rather than restore sight, and they are not right for everyone, so they are a conversation to have with a retina specialist. The larger point is that "there's nothing to do" is out of date. There is almost always something, and the earlier the diagnosis, the more the options are worth.
Myth: Low Vision Means the End of Independence
Perhaps the most quietly harmful myth is that once central vision fades, a person can no longer live on their own terms. In reality, most people with AMD keep living at home and doing the things that matter, with some adjustments and the right support. Low-vision rehabilitation, high-powered magnifiers, screen readers, talking clocks and watches, large-print books, and simple changes like brighter, glare-free lighting and high-contrast tape on stair edges all extend independence considerably.

Where sight limits the small tasks of a day, a bit of human help fills the gap without taking over. Reading the mail and medication labels, driving to eye-injection appointments, sorting the pillbox, and keeping walkways clear are exactly the kinds of things a caregiver can handle so vision loss does not become a safety problem. Families we work with often pair low-vision tools with companion care for reading, errands, and rides to appointments, or with personal care when daily routines like cooking and grooming have gotten harder to manage safely. Across our Monmouth County, New Jersey service area and beyond, that kind of steady, practical support is often what lets someone with AMD stay in the home they love. Because vision changes also raise the risk of falls, it is worth pairing it with the fixes in our guide to bathroom safety for seniors.
What the Facts Add Up To
Strip away the myths and macular degeneration becomes something a family can face clearly instead of dread. It usually spares side vision, so total blindness is rare. Its biggest risk factors, especially smoking and blood pressure, are partly in your hands. Dry and wet are different diseases with different plans. It hides early, which is exactly why the yearly dilated exam and the Amsler grid on the fridge are worth the small effort. And treatment, from injections to supplements to low-vision support, keeps getting better.
The single thread running through all of it is early detection. The sooner AMD is caught, the more vision there is to protect and the more the treatments are worth. If someone you love is noticing wavy lines, a dim central spot, or that reading suddenly takes more light, do not wait to see if it passes. Book the eye exam, and know that whatever the result, keeping them safe, independent, and at home is very much still on the table.
This article is general information, not medical advice. Symptoms, risk factors, and treatments vary by person, and AMD care changes over time; talk with an eye doctor or retina specialist about diagnosis and the options that fit your situation.
Frequently Asked Questions
Does macular degeneration always lead to blindness?
No, and this is the biggest misunderstanding about the disease. Macular degeneration damages the macula, which handles sharp central vision, but it leaves the peripheral retina largely intact. That means even someone with advanced AMD usually keeps the side vision they need to walk through a room, sense movement, and stay oriented. What people lose is the fine detail in the center of their gaze, which makes reading, driving, and recognizing faces harder. Legal blindness is possible in advanced cases, but complete darkness is rare. The realistic picture is manageable low vision, not total blindness, and how much a person keeps depends heavily on catching it and treating it early.
What is the difference between dry and wet macular degeneration?
Dry AMD is the common, slow form. It accounts for roughly 80 percent of cases and develops as the macula gradually thins and small yellow deposits called drusen build up. Vision usually fades over years, not weeks. Wet AMD is less common but far more aggressive: abnormal blood vessels grow under the retina and leak fluid or blood, which can distort and damage central vision quickly, sometimes within days. Wet AMD is responsible for most of the severe vision loss from the disease. Dry AMD can also turn into wet AMD, which is one reason regular monitoring matters. The good news is that wet AMD is the more treatable of the two, thanks to eye injections that can halt and sometimes reverse the damage.
What are the first signs of macular degeneration?
Early AMD is often silent, but the first noticeable changes tend to show up in central vision. Straight lines, like door frames or the edges of a page, may start to look wavy or bent. A blurry or dim spot can appear in the middle of your view while the edges stay clear. Colors may seem less vivid, and reading or seeing faces may need much brighter light than before. Because one eye often compensates for the other, these changes can go unnoticed until they are advanced, which is why covering one eye at a time to check each one separately, and using an Amsler grid at home, is so useful.
Is macular degeneration hereditary?
Family history is one of the strongest risk factors for AMD, so genetics play a real role. If a parent or sibling has the disease, your own risk is higher, and researchers have identified specific gene variants tied to it. But heredity is not destiny. AMD develops from a mix of genes, age, and lifestyle, and several of the biggest contributors are things you can influence, especially smoking, blood pressure, and diet. Someone with a family history who does not smoke, eats well, and gets regular dilated eye exams is in a far better position than the genes alone would suggest.
Can macular degeneration be prevented?
There is no guaranteed way to prevent AMD, but you can meaningfully lower the risk and slow it down. Not smoking is the single most powerful step, since smoking roughly doubles the risk. Keeping blood pressure and weight in a healthy range, eating leafy greens and fish, exercising, and protecting your eyes from strong sunlight all help. For people who already have intermediate AMD, a specific supplement formula called AREDS2 can slow progression to the advanced stage. Prevention is really about stacking these odds in your favor and catching any changes early with regular eye exams.
Do AREDS2 vitamins actually help with macular degeneration?
For the right person, yes, but with an important limit. The AREDS2 formula is a specific combination of antioxidants and minerals, including vitamins C and E, zinc, copper, lutein, and zeaxanthin, studied in large national trials. It has been shown to slow the progression from intermediate AMD to the advanced, vision-threatening stage. What it does not do is prevent AMD in people who do not have it, restore vision that is already lost, or help those with only early disease. It is not the same as an ordinary multivitamin, either. Anyone considering it should confirm with an eye doctor that they are at the stage where it helps.